An MCQ based case discussion by
Dr. Spoorthy Gurajala, MD, DNB, Manipal Hospital, Bangalore
CASE HISTORY
A 50-year-old woman presented with hematuria. Imaging showed a posterior bladder wall mass, and cystoscopy revealed an irregular lesion suspicious for malignancy, prompting TURBT
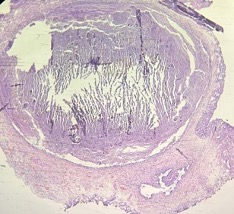
These are the H&E images -
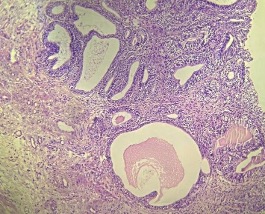
MCQ 1
What is your first impression?
A. High-grade invasive carcinoma
B. Benign glandular/cystic lesion
C. Suspicious for malignancy
D. Pure inflammatory lesion
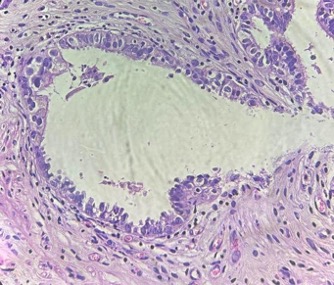
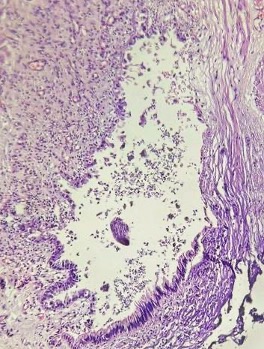
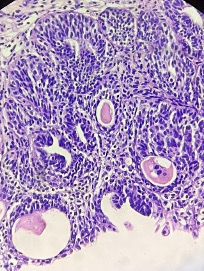
On higher magnification:
Some glands are dilated and filled with secretions
Others are lined by:
Ciliated columnar epithelium
Endocervical-type mucinous epithelium
MCQ 2:
What does this epithelial pattern suggest?
A. Urothelial differentiation
B. Intestinal metaplasia
C. Müllerian differentiation
D. Nephrogenic adenoma
CK7
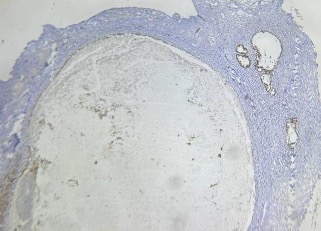
ER
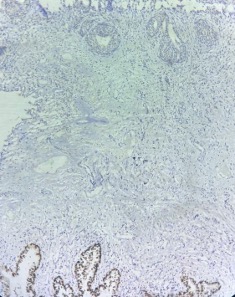
PAX-8
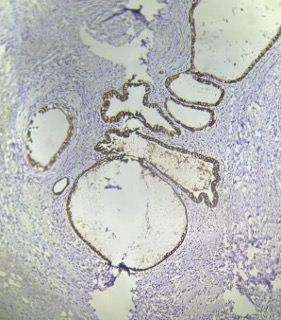
IHC shows:
PAX8 positive
ER positive
CK7 positive
MCQ 3
This immunoprofile supports:
A. Urothelial carcinoma
B. Colorectal adenocarcinom
C. Müllerian origin
D. Renal origin
------------------------------------------------------------------
31 March 2026:
Answers:
MCQ 1 - Answer: B
MCQ 2- Answer: C
MCQ 3 - Answer: C
Discussion
Müllerinosis is a rare benign choristomatous lesion characterized by the presence of an admixture of two or more Müllerian-derived tissues—namely endometriosis (endometrial glands with stroma), endosalpingiosis (ciliated tubal-type epithelium), and endocervicosis (mucinous endocervical-type glands)—occurring in an ectopic location, most commonly the urinary bladder. It is thought to arise from developmental misplacement of Müllerian duct remnants, although metaplastic transformation of coelomic epithelium has also been proposed.
Clinically, it typically affects women of reproductive age and may present with cyclical hematuria, dysuria, or pelvic pain, often mimicking a bladder neoplasm on imaging and cystoscopy.
Histologically, the lesion is located in the lamina propria or muscularis and shows a benign admixture of Müllerian components without cytologic atypia or destructive invasion. Immunohistochemistry demonstrates positivity for ER, PR, and PAX8, with CD10 highlighting the endometrial stromal component. The main differential diagnoses include isolated endometriosis, cystitis glandularis, nephrogenic adenoma, and primary adenocarcinoma of the bladder, the latter distinguished by cytologic atypia and invasive growth.
Müllerinosis is a benign condition with an excellent prognosis, and complete local excision is usually curative.

B,C,C
Nephrogenic adenoma
MCQ 1: B. Benign glandular/cystic lesion
MCQ 2:C. Müllerian differentiation
MCQ 3:C. Müllerian origin
1.C. Suspicious of malignancy
2. C. Mullerian origin
3. C. Mullerian origin
Muller Ian oigin
MCQ 1B. Benign glandular/cystic lesion.MCQ 2:C. Müllerian differentiation.MCQ 3C. Müllerian origin
MCQ-1-B
MCQ-2-C
MCQ-3-C